I hope most of the people who are reading this article might have heard the term many times in your daily OPD. The first time I saw a case of Dentigerous Cyst was when I was working in a clinic and a patient came with severe swelling in the lower right back tooth region.
In this article, I will discuss in detail about Dentigerous cyst so that it will be useful for you.
Before going to the Dentigerous cyst, let me discuss what is a Cyst.

Contents
WHAT IS A CYST?
You all are familiar with the term cyst. We can define it as”A pathologic cavity having fluid, semi-fluid, or gaseous content but not always lined by epithelium”.
Most of the time the main discomfort felt by the patient is pain. Due to this pain in most cases, the patients approach the clinic. It also can be some swelling or any other discomfort.
The symptoms of a cyst include, generally the patient comes with pain and swelling in the jaw. In some cases, the patient experiences paresthesia or anesthesia. The taste changes to salty and tooth discoloration can also be seen.
Now let’s discuss about Dentigerous Cysts.
As this article is mainly read by dental students or practitioners you all are familiar with the term Dentigerous cyst. The patient mainly 18 to 20 years of age comes with a swelling in the jaw and when we observe clinically there will be a missing tooth.
The term dentigerious cyst is also known as follicular cyst or pericoronal cyst. It is the most common type of odontogenic [means arising within the tooth or surrounding tissue] cyst seen in the crown of an unerupted tooth.
As they are seen in the unerupted tooth, this helps us to identify with the help of a radiograph as the tooth will be missing, altered, or misaligned.
WHAT ARE THE CLINICAL FEATURES?
As we discussed earlier it arises from the follicle of an unerupted tooth. They are commonly seen in children and adolescents. Where do you see it? They are commonly seen in the mandibular third molar and maxillary canine which is the most commonly impacted tooth.
The dentigerous cyst is generally painless but it becomes painful once it is infected. As it expands it will go and compress the sensory nerves which results in pain and gets referred to other areas.
When we talk about the size of the cyst the diameter will be more than the size of the tooth. As it gets enlarged the neighboring tooth gets displaced or moved out of the arch and gets resorbed.
In some cases, the third molar gets displaced in such a way that it will compress the inferior border of the mandible.
Due to the compression, there will be pathological fractures.
The hollowing out of the ramus takes place which extends to the coronoid process and condylar process and the body causing expansion of the cortical plates.
If the cyst is associated with the maxillary cuspid there will be an expansion of the anterior maxilla and it resembles cellulitis and sinusitis [it is a condition characterized by inflammation of the paranasal sinus].
The dentigerous cyst is associated with some syndromes like BASAL CELL NEVUS SYNDROME, and CLEIDOCRANIAL DYSPLSAIA.
In some cases, the cyst contains blood in it then it’s called as Blue Domed Cyst.
WHAT ARE THE COMPLICATIONS?
If the dentigerous cyst is not removed properly or incompletely removed it results in certain potential complications such as Ameloblastoma and mucoepidermoid carcinoma. So, the surgical treatment should be done with an efficient and experienced surgeon.
The mucoepidermoid carcinoma is a tumor of the salivary gland associated with the lining epithelium. So, as it spreads it affects the salivary glands too.
HOW IT APPEARS RADIOGRAPHICALLY?
The radiographic examination includes a well-defined radiolucency with a hyperostotic border [which means abnormal enlargement of the outer layer of the bone].
Usually, when we observe radiographically, they are unilocular but in some cases, they appear multilocular.
When we observe the margin, they are well-defined and if they are infected they appear ill-defined.
HOW IT APPEARS IN THE TEETH?
In the teeth, it envelops the crown symmetrically and expands laterally.
Where does the cyst get attached?
The cyst gets attached in the cementoenamel junction and the gets expanded in the apical direction.
As we mentioned before they are commonly seen in the mandibular molar and the maxillary canine region. The larger cyst is commonly seen in the mandibular area.
The root of the tooth and adjacent tooth gets resorbed.
The dentigerous cyst is commonly unilateral but, in some cases, they are seen bilateral also. We can also find multiple dentigerous cysts in one patient.
WHAT ARE THE RADIOGRAPHIC TYPES?
When we observe radiographically there are different types of dentigerous cysts.
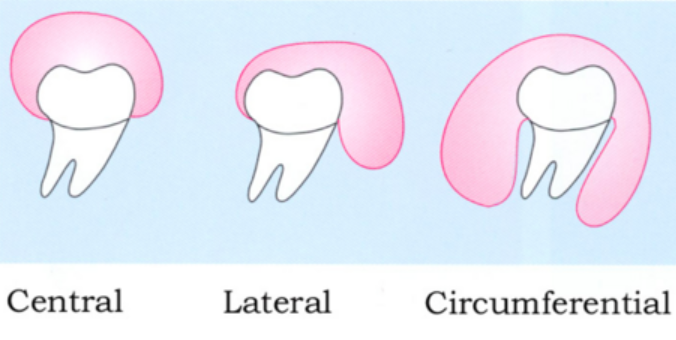
Central variety:
In this case, the crown is enveloped symmetrically. The pressure will be applied to the crown of the tooth and this results in the eruption of the tooth away from its direction. In such cases, the third molar may be found on the lower border of the mandible and in the ramus. In the same way, the maxillary canine can be seen in the sinus or on the floor of the orbit.
Lateral type
In this type of dentigerous cyst when we observe radiographically there will be dilation of the follicle in one aspect of the crown.
Where do you see such a type of cyst?
Such type of cyst can be seen in partially erupted teeth.
Circumferential type:
In this type of dentigerous cyst, the entire tooth appears enveloped by the cyst.
HOW WILL YOU DIAGNOSE THE DENTIGEROUS CYST?
Clinical diagnosis
When the patient comes to your clinic first you should observe clinically. There will be expansive swelling in the posterior region of the mandible. This is a clue for dentigerous cysts.
Radiographic diagnosis
After the clinical examination, the next procedure is will ask the patient to go for a radiograph.
As we discussed earlier the radiographic examination shows a well-defined radiolucency associated with these impacted tooth teeth with a hyperostotic border and well-defined margin that tells that it’s a dentigerous cyst.
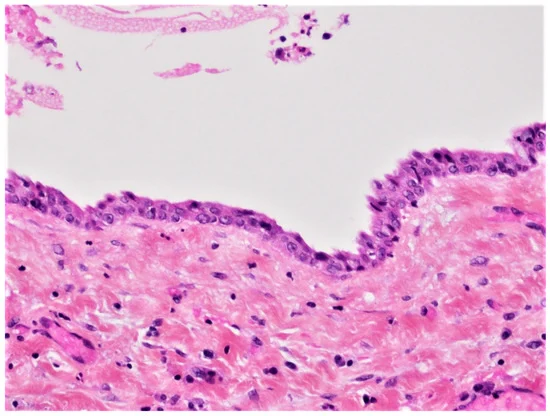
Laboratory diagnosis:
For laboratory diagnosis first, we need to do a biopsy. The biopsy result shows a thin connective tissue wall with a thin layer of stratified squamous epithelium lining the lumen. The rete pegs formation is absent. The Rushton bodies are present. Also, fluid can be aspirated from this lesion.
HOW WILL YOU MANAGE DENTIGEROUS CYST?
The management of dentigerous cysts includes surgical treatment.
The smaller cyst can be removed surgically and the larger cyst removal needs drainage of the cyst and marsupialization. This helps us to relieve pressure and results in shrinkage of the cyst.
There is another treatment called the decompression technique in which a small acrylic button or short section of rubber is placed in the preferred surgical opening which helps with drainage and keeps the cyst open.
In this case, the recurrence of the cyst is less unless the fragments of the cystic lining are allowed to remain.
CONCLUSION
As a part of the conclusion, I conclude that the dentigerous cyst is commonly seen in the unerupted tooth. It is also known as follicular or pericoronal cyst. It is painless, the teeth get displaced, resorbed, and pathologically fractured. When the cyst contains blood in it the is known as blue domed cyst.
There are certain complications of this cyst as it causes ameloblastoma which is a malignant condition, and mucoepidermoid carcinoma which affects the salivary glands. When we observe clinically seen in unerupted teeth the radiographic examination is a must.
The radiographic appearance shows unilocular radiolucency with hyperostotic borders and resorption of the tooth can also be seen. The management of the cyst includes surgical treatment with surgical drainage, marsupialization, and decompression followed by orthodontic treatment.
You might have heard the term Eruption cyst along with Dentigerous Cyst. I have written a detail article about the same.
Got some question?
If you are having any questions, then feel free to comment it below and revert back as soon as possible.
If you loved this article, then please do share it with your friends and students in need. 😀